How the patient experience adds value to hospitals
March 2026

Time for a broader perspective in the design process
Every healthcare provider wants to deliver good care, and every patient wants to receive good care. We all know that good care is about more than medical procedures and technology. It is the interplay of people, processes and the physical environment that ultimately determines the quality of care.
But how does the patient actually perceive care? How does one “know” whether the care they have received is actually good? Our perceptions are strongly influenced by our experience. By what we see, hear, smell, feel and taste – in short, by our senses and the emotions that arise from them.
Various studies clearly show that the environment in which care is provided has a major impact on the patient’s health and well-being. A sick person is bound to experience the hospital environment differently than a healthy one. Feelings of fear and uncertainty, for example, can make stimuli feel more intense. In other words, an environment that reduces fear and stress is also one that stimulates recovery. What’s more, a positive environment and experience can compel patients to rate a hospital more highly and make them more likely to recommend it to others.
As architects, we give spatial form to the path of diagnosis, treatment, healing, or processing and acceptance every day. Still, we wonder whether we truly have sufficient insight into how patients actually experience the hospital. This raises an interesting but also fundamental question:
Can we design better hospitals by taking the patient’s perspective more actively into account?
In this research report, we would like to share our ideas on this subject with you, with the aim of really put the patient first, to make them feel heard and ensuring that their perspective is reflected in the final hospital design.

Process- and patient-oriented design
Traditionally speaking, most hospitals are designed with processes in mind. However, as healthcare designers, we have long focused on creating an integrated building environment that positively influences the experience of all users.
We recognise the significant added value of a healing environment – not only for patients, but also for healthcare providers and visitors. That said, complex logistics, efficient work processes and optimal routing of people and equipment remain essential. But the question is: are we truly considering the patient’s perspective in these essential processes, or is there still room for improvement?
‘Patients first’
An increased focus on patient-centred design might seem obvious. Nowadays, every hospital claims to put the patient first. But is that true? If you dare to take a critical look, are you really putting the patient first? In practice, the patient is not always as central as we would like them to be.
If you really want to put the patient first, there are roughly two ways to go about it.
- Make the patient central to the design, and organise processes around them. An example of this approach is the so-called Mamma clinic, where functions that are normally spread across the hospital (imaging, functional examination rooms and consultation rooms) are clustered in a single area. This concept reduces stress for the patient and increases satisfaction (e.g. diagnostics in one day, multidisciplinary appointments), ultimately benefitting the hospital. This tightly structured care process simplifies the “care pathway”, resulting in an innovative floor plan, like the one at Amphia Hospital in Breda. This “one-stop shop” strategy is being used more and more frequently, for example in the cardiology departments of various hospitals, such as Spaarne Gasthuis and Tergooi MC.
- Consider the patient’s value judgement as the starting point, and make design decisions are based on that. An example of this is the children’s advisory board found at various hospitals, which contributes ideas about elements that children consider important. Another example is the value-driven care concept, which attempts to tailor care to the patient’s needs. In practice, however, we often see that patient input is only minimally involved in the development of the Programme of Requirements and therefore has limited influence on guiding decisions.
Everything in context
A hospital is a complex environment. As an architectural firm focused on healthcare, we know that all aspects must be viewed in context. There is a wide variety of patients, and each patient has their own care pathway. The example of the Mamma clinic, where care processes had to be radically changed, also shows the impact that such changes can have on healthcare, because they require a completely different way of working. Sometimes there are conflicting interests. Nevertheless, we believe that the interests of patients and professionals can be united in efficient, future-proof care processes and concepts.

Incorporating patients' value judgements into the design
At Wiegerinck, we listen carefully to the desired care processes and are fully aware of the fact that we can’t change everything. In many cases, we become involved in the design process after the Programme of Requirements has already been drawn up. At that point, it can be difficult to maintain sufficient focus on the patient. In regular design meetings, there is not always room for direct patient input. As architects, we are able to use our experience and research to identify issues and safeguard the patient experience; however, we feel that this isn’t always enough. That’s why we have developed an alternative approach. An approach in which the patient’s voice is heard. We collect their value judgements and opinions and incorporate this knowledge into the design.
Based on key sources
Our design approach is based on proven principles and key sources. For example, we can to tap into our existing research in Evidence-Based Design and our knowledge of environmental psychology. Additionally, we can draw from another industry we work in: hospitality. How are users’ value judgements incorporated into the design process in the hospitality industry?
What hospitality teaches us
Hospitality is a world where (online) reviews can make the difference between success and failure. In the hotel industry, the word hospitality is a core concept, and we are increasingly seeing this as a core value in hospitals as well: hospitality and a positive attitude. Hospitality is about creating a warm, welcoming feeling for everyone who enters a space. It goes beyond simply providing service; it is about consciously responding to the needs and wishes of guests. By providing attention, a personal approach and excellent care, you not only meet practical and functional expectations, you exceed them.
Systematic analysis, then (re)design
Hotel chains develop knowledge by systematically analysing guest feedback. Designers are then tasked with translating this feedback into spatial interventions: from the positioning of the bed in relation to the window to the acoustics in corridors and lobbies. These adjustments are not random but based on user experiences. The hotel industry shows us just how powerful it is to put experiences at the heart of design and service choices. Thinking and improving based on experience offers valuable lessons for the design of hospitals.
The Wiegerinck approach: translating experiences into an experience route
In our approach, we think from the perspective of a specific patient group or care pathway. To do so, we collect input from a specific group of patients. Examples include outpatients undergoing a functional examination, patients coming to in the treatment centre for endoscopic research, or geriatric patients in general. Using an easy, accessible questionnaire, we ask them to fill in their own care pathway with information about their route, duration and experience; we call this an experience route. From there, we distil the common denominator and the striking deviations per group. We can then implement these findings into the design process and take them into account as important decisions are made.
Starting with a representative group
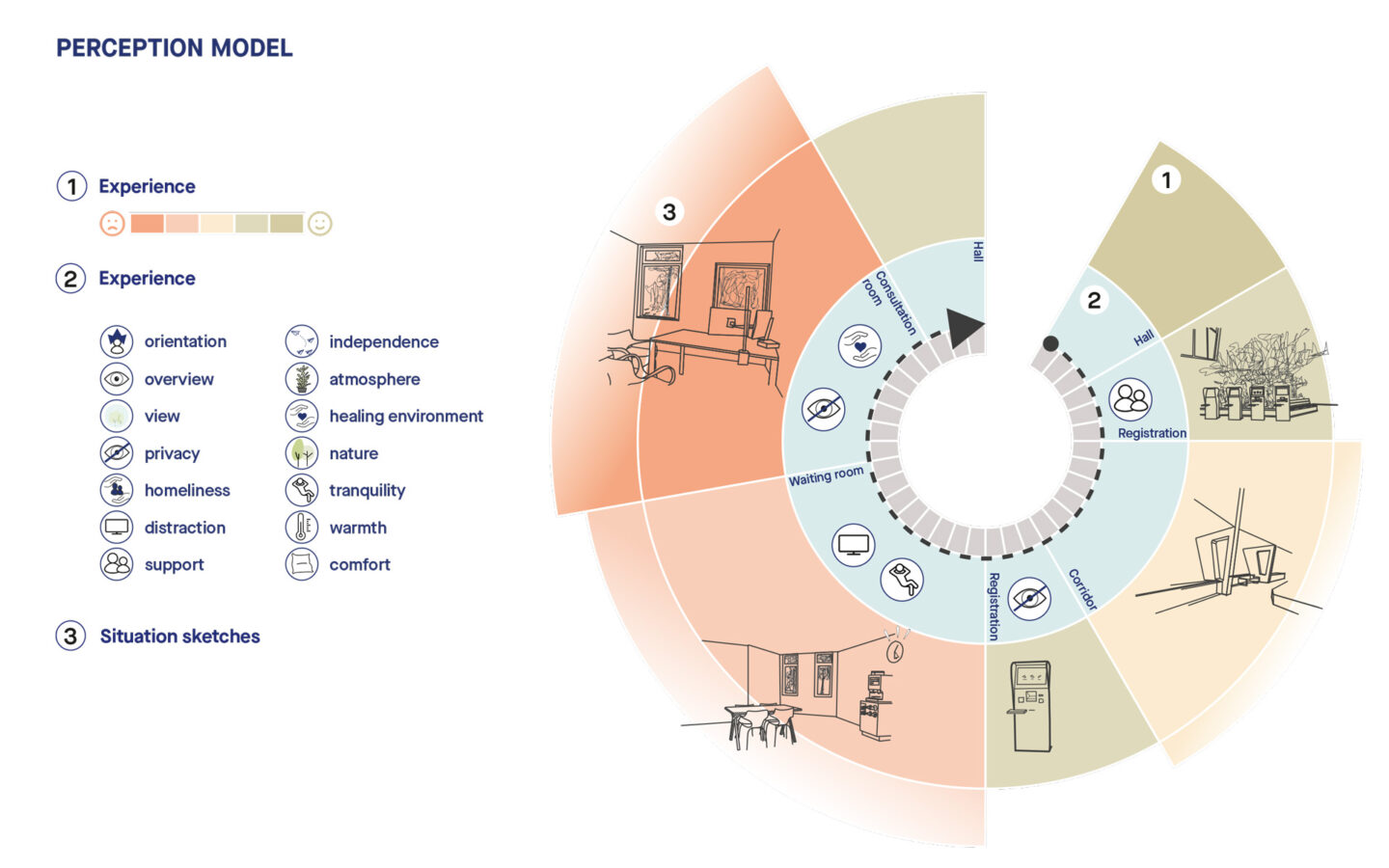
For our research, we created an experience route based on interviews with several diabetes patients. Diabetes patients form a large, representative group of chronic patients who visit the hospital regularly. Using our model, we recorded their “care pathway” through the hospital and delved deeper into their emotions, experiences and perception of spatial aspects. This resulted in an experience route that provides insights into the order in which the rooms are visited, how long a patient stays in a particular place, how the patient feels in that space and how the spatial aspects of it are experienced.
It is essential that the questionnaire be filled in by a patient or a family member, rather than by a healthcare professional. In this way, we avoid interpretations that may be influenced by divergent interests.
Development of the model
In order to process the interviews in a targeted manner, we have developed a model of the experience route that we can fill in for each interview via a questionnaire. This allows us to grow our knowledge base. We can tailor this model to specific projects, use it during workshops with patients, and utilise the output throughout the entire design process, from the Programme of Requirements to user consultations. The resulting knowledge and insights enable us to design a more suitable environment. In short, this process allows us to provide maximum support to the hospital for specific tasks.
In addition to this approach, we believe that a patient council should be involved as early as the Programme of Requirements phase. From the outset, this council can act as a sounding board for specific patient-related topics. It would also be valuable to consult a delegation of patients more frequently on specific themes during the early design phases, for example in the form of workshops.
This involvement can provide valuable insights, draw attention to under-exposed topics and contribute to greater satisfaction with the end result. It can also ensure understanding and insight when it comes to weighing of interests.
Shaping the best care together
In any hospital, care revolves around sincere attention to the well-being of others. By creating a pleasant, well-designed environment, we can significantly improve the patient experience. Evidence-Based Design shows that such an environment reduces anxiety and stress, thereby supporting the healing process. The experience route helps to visualise the essence of care – as seen through the eyes of the patient.
Together with you, we want to give the patient’s voice a central place in the design of the care environment. We hope that our research will inspire you to consider the possibilities with us and continue the conversation.